Myopathies (muscle disorders) for undergraduate
0 likes412 views

herediatary myopthies myotonia inflammatory myopthies

































































More Related Content
Similar to Myopathies (muscle disorders) for undergraduate (20)
More from Mohamed Rizk Khodair (20)


















Recently uploaded (20)












Myopathies (muscle disorders) for undergraduate
- 1. Myopathies Dr mohamed rizk khodair [email protected] Lecturer of neurology
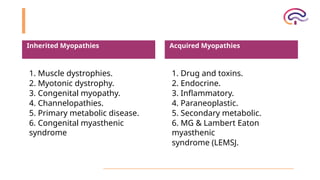
- 2. Inherited Myopathies 1. Muscle dystrophies. 2. Myotonic dystrophy. 3. Congenital myopathy. 4. Channelopathies. 5. Primary metabolic disease. 6. Congenital myasthenic syndrome Acquired Myopathies 1. Drug and toxins. 2. Endocrine. 3. Inflammatory. 4. Paraneoplastic. 5. Secondary metabolic. 6. MG & Lambert Eaton myasthenic syndrome (LEMSJ.
- 3. General clinical picture of myopathies 1- weakness : • usually affects proximal muscle group ( shoulder and limb girldes ) • Selective to certain muscle • In neonatal peroid hypotonia ( floopy infant) syndrome • In later infance and childhood delay motor milestones • +/- cranial muscle affections : facial , bulbar and extraocular • +/- Special signs : winging of scapula ( weak serratus anterior ), beevor sign • Trunk muscle weakness : pot-belly abdomen , lumber lordosis • Gower’s phenomena : climbing himself during standing • Assosciated with hypotonia and atrophy ( relatively late ) +/- pseudohyperatrophy • Waddling gait NB : All muscles diseases affected proximal > distal except distal myopathies , myotonia dystrophica & inclusion body myositis
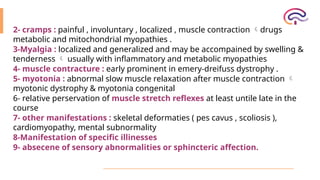
- 5. 2- cramps : painful , involuntary , localized , muscle contraction drugs metabolic and mitochondrial myopathies . 3-Myalgia : localized and generalized and may be accompained by swelling & tenderness usually with inflammatory and metabolic myopathies 4- muscle contracture : early prominent in emery-dreifuss dystrophy . 5- myotonia : abnormal slow muscle relaxation after muscle contraction myotonic dystrophy & myotonia congenital 6- relative perservation of muscle stretch reflexes at least untile late in the course 7- other manifestations : skeletal deformaties ( pes cavus , scoliosis ), cardiomyopathy, mental subnormality 8-Manifestation of specific illinesses 9- absecene of sensory abnormalities or sphincteric affection.
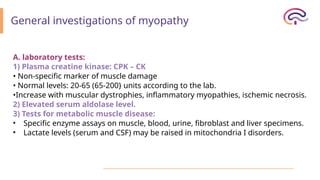
- 6. General investigations of myopathy A. laboratory tests: 1) Plasma creatine kinase: CPK – CK • Non-specific marker of muscle damage • Normal levels: 20-65 (65-200} units according to the lab. •Increase with muscular dystrophies, inflammatory myopathies, ischemic necrosis. 2) Elevated serum aldolase level. 3) Tests for metabolic muscle disease: • Specific enzyme assays on muscle, blood, urine, fibroblast and liver specimens. • Lactate levels (serum and CSF) may be raised in mitochondria I disorders.
- 7. B- electrophysiological studies • They help exclude neurogenic and neuromusclar junction disorders . • Useful in determining whether a neuropathic , myopathic or mixed disorder. • In patient with pure muscle disease , sensory and motor nerve conduction unremarkable • Electromyography is important for specific muscle myopathies
- 8. C- genetic analysis • Fisrt line investigation for many genetic muscle diseases ( musclar dystorphies , myotonia and mitochondrial ) D- muscle biopsy : open or needle biopsies E-imaging • MRI detects subclinical changes and pattern of muscle involvement • Muscle ultrasonography : usfel and noninvasive
- 9. Muscular Dystrophy Muscular dystrophies (MDs) It is a group of primary inherited degenerative and progressive myopathies, affecting skeletal muscles, with muscle biopsy of degeneration and regeneration of muscle fibers only.
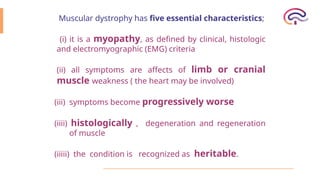
- 10. Muscular dystrophy has five essential characteristics; (i) it is a myopathy, as defined by clinical, histologic and electromyographic (EMG) criteria (ii) all symptoms are affects of limb or cranial muscle weakness ( the heart may be involved) (iii) symptoms become progressively worse (iiii) histologically , degeneration and regeneration of muscle (iiiii) the condition is recognized as heritable.
- 11. Classification of Muscular Dystrophies 1-X- linked muscular dystrophies • Duchene muscular dystrophy • Becker(benign) muscular dystrophy • emery dreifuss 2 –Autosomal recessive muscular dystrophies • Scapulohumeral • distal myopathies • congenital • Limb girdle type 2 3–Autosomal dominant muscular dystrophies • Facioscapulohumeral • scapuloperoneal • myotonia dystrophica • Limb gridle type 2
- 12. Another Classification of Muscular Dystrophies Dystrophinopaties Duchene muscular dystrophy Becker muscular dystrophy Non Dystrophinopaties Emery Dreifuss muscular dystrophy Facioscapulohumeral muscular dystrophy Limb- girdle syndromes Congenital muscular dystrophy ( and Fukuyama type) Myotonic dystrophy Extraocular muscle specific dystrophy
- 14. Duchenne Muscular Dystrophy Most common muscular dystrophy encountered Incidence 1: 3,500 live male births X-linked disorder DMD gene isolated to short arm of the X chromosome at position 21. 60% of dystrophin mutations are deletions whereas approximately 40% are point mutations.
- 15. DMD gene product: dystrophin Absent or nonfunctional in DMD patients --- sequence of events occurs that leads to --> muscle cell membrane degeneration and death Dystrophin provides strength to muscle cell by linking internal cytoskeleton to the surface membrane.
- 16. Clinical manifestation of Duchenne Muscular Dystrophy • It affects boys and starts in early childhood (between 2 and 5 years). • Distribution usually starts in pelvic girdle delayed walking and other motor milestones, difficulty in running, climbing the stairs, Gower maneuver, and affection of • shoulder muscles soon follows 7 rapidly progressive, the patient cannot walk by the age of 12 years . • pseudohypertrophy in the calves, vastus lateralis, and deltoids. • Others : skeletal deformities (pes cavus, kyphoscoliosis), cramps, contractures (late); cardiomyopathy, deep Q wave, tall R-wave, on ECG, arrhythmias, and mental sub normality
- 18. A 7-year-old boy presents with progressive weakness of both legs for 4 years.
- 20. Child with Duchenne muscular dystrophy; note the calf hypertrophy, mild equinus posturing at the ankles, shoulder retraction, and mild scapular winging.
- 21. Gowers’ Maneuver
- 22. Gower’s sign in a seven-year-old boy with Duchenne muscular dystrophy
- 23. Myopathic gait pattern in DMD due to pelvic girdle and knee extension weakness; a) lumbar lordosis to keep center of mass posterior to hip joint; anterior pelvic tilt due to hip extensor weakness; weight line/center of mass maintained anterior to an extended knee; and forefoot ground contact with stance phase plantar flexion (toe walking) to maintain a knee extension moment and knee stability; b) trendelenberg or “gluteus medius gait” with lateral lean over the stance side due to hip abductor weakness; ankle dorsiflexion weakness necessitates swing phase circumduction for clearance.
- 24. Diagnosis A) Clinical picture B) Increase in serum CK (creatine phosphokinase) levels up to 10 times normal amounts. C) EMG &NCV -- myopathic features. D) Muscle biopsy--- myopathic or dystrophic features E) Immunohistochemstry-- specific deficient protein as dystrophin gene protein. F) Genetic testing--- dystrophin gene deletion or mutation.
- 25. Treatment of Duchenne • In DMD corticosteroids (deflazacort ) muscle strength, muscle mass, ↑ ↑ progression. Mechanism unknown; may be due to muscle protein ↓ ↓ degradation rather than immunosuppression.Recommended starting dose in ambulatory boys 0.75 mg/kg daily (maximum dose 40 mg) Azathioprine and cyclosporin no benefit. • Exon skipping : eteplirsen • Gene therapy : ataluren • Ventilatory support increases quality of life and life expectancy.
- 26. Becker Type, BMD: o later age of onset (5-25 years}, milder form. o Slowly progressive, still walking beyond 16 years .old .. o Pseudohypertrophy may occur, and muscle cramps are common. o No skeletal deformity or mental subnormality. o less cardiac affection (only 40%).
- 27. Facioscapulohumeral Muscular Dystrophy • It is an autosomal dominant slowly progressive muscular dystrophy usually of benign course, affecting the musculature of the face and shoulders . • Clinically, the age of onset is usually between 6 to 20 years . • The first manifestations are difficulty in raising the arms above the head and winging the scapulae . • There is involvement specially of the orbicularis oculi, zygomaticus, and orbicularis oris muscles inability to close the eyes firmly, to purse the lips and to whistle . • It has a characteristic descending pattern of weakness, start in the .face and shoulder , followed by the distal lower extremity (weak ankle dorsiflexors) and the proximal hip girdle muscles. • Weakness may be asymmetrical; deltoids are usually preserved. • Polyhill appearance, Beevor sign, Popeye arm appearance with protrusion of buttocks. • No ptosis or extraocular muscle involvement , cardiac affection or mental retardation, No skeletal deformities and contractures.
- 28. Facial weakness of orbicularis oculi in Facioscapulohumeral Muscular Dystrophy (FSHD). Eye closure is weak and weakness of orbicularis oris produces difficulty smiling, puffing out the cheeks, and pursing the lips
- 29. Winging scapula Markedly decreased shoulder flexion & abduction Horizontal clavicles Forward sloping Rare scoliosis
- 30. Limb girdle muscular dystrophy • A heterogeneous group of progressive disorders mainly affecting the pelvic and shoulder girdle musculature . • Sever forms & milder forms . • Autosomal recessive (more common & more severe) and dominant forms.
- 31. Myotonic Dystrophy General criteria for myotonia : • Characterized by slowing of relaxation of skeletal muscles after voluntary contraction improves by warmth and exercise and worsen by cold and rest. • Inherited as autosomal dominant. Myotonic phenomena is provoked by gentle percussion on muscles ( as thenar muscles ). • EMG shows dive bomber sound with insertion of the needle into muscle. • Phenytoin, procainamide, quinidine, may alleviate myotonic phenomena by delaying membrane excitability. • Two types: myotonia atrophica & myotonia congenita
- 32. A) Myotonia Atrophica Onset: middle-aged male; there are diminished fertility and increase infantile mortality rate. Clinical Picture: 1. Facies: ptosis (LPS), Squint (EOMs}. · o Wasting of masseter, sternomastoid, and temporalis. o long face, mournful expression, premature balding. o Hallow and echoing voice. 2. Limbs: weakness and wasting of distal muscles of UL (forearm, fingerflexors) and LL o Muscles wasting are due to selective reduction of protein synthesis.· 3. Eyes: 90% of cases cataract. VEP is abnormal. 4. Ear : sensory neural deafness. 5. Heart: myopathy, prolapse of mitral varve, conduction defect. 6. Chest: poor: pulmonary functions test so tolerate barbiturate anesthesia poorly. 7. G/T: hypersomnia,. esophageal contractility disorders, smooth muscles of colon disorders & constipation. 3. Testis: atrophy. 9. Ovaries: irregular menstruation ~infertility. 10. Mentality: cognitive deficits. 11.Excessive daytime sleepiness with respiratory muscle weakness. 12. Diabetes mellitus. 13. Myotonia: delayed relaxation, due to repetitive discharge of muscle fiber.
- 33. Characteristic Appearance - MD
- 34. B) Myotonia Congenita (Thomsen Disease) o Heredity: AR or AD, due to mutation of gene of cl channels on chromosome 3. o Appears in first and second decades; in females more than males. o Pathophysiology: decreased Chloride (CI) conductance Clinical Picture: • Generalized myotonia in most muscles. • It is provoked by exertion following rest and improved by exercise. • Muscle hypertrophy in most muscles (Hercules faces). • Transient weakness. • No dystrophic changes.
- 35. Idiopathic inflammatory myopathies 1. Polymyositis 2. Dermatomyositis 3. Inclusion body myositis 4. Myositis associated with malignancy
- 36. Idiopathic inflammatory myopathies • group of acquired diseases characterized by inflammatory infiltrate of skeletal muscle. • Potentially treatable. • Sex: females more than males • Preceding factors: usually spontaneous, may follow fever, drugs, exposure, to sun (dermatomyositis). • Acute, subacute, or chronic course. • Criteria to define polymyositis & dermatomyositis : 1. Symmetric weakness of limb girdle muscles and anterior neck flexors. 2. The weakness is progressive over weeks to months with or without dysphagia or respiratory muscle involvement. 3. Elevation of levels of serum skeletal muscle enzymes (CK, aldolase, AST/ALT and LDH) triad of short, small polyphasic motor units; fibrillations, positive waves, and insertional irritability; and 4. Electromyographic (EMG) bizarre high-frequency discharges. 5. Dermatologic features (in dermatomyositis) including a heliotrope rash with periorbital edema; a scaly, erythematous dermatitis over the dorsa of the hands, especially over the MCP and PIP joints (Gottron's sign); and involvement of the knees, elbows, medial malleoli, face, neck, and upper torso.
- 37. Clinical Manifestations 1) General criteria of myopathy are present. 2) Specific manifestations: o Pain and tenderness of the muscles in 50% of cases. o Dysphagia, weakness of neck muscles (extensors) occur early, rarely facial or ocular manifestations. o Respiratory muscle affection may occur. o Deep reflexes are usually depressed o o Muscles atrophy only in chronic cases . 3) Systemic manifestations: malaise, arthralgia, Raynaud's phenomenon, myocarditis, interstitial lung disease. 4) In Dermatomyositis: • Erythematous patches or exfoliative lesions with discoloration of the cheeks, nose and forehead (heliotrope). • May proceed, associate or follow myositis. • In butterfly distribution, exposed V shaped, extensor surface of knuckles, knees, elbows, Gottron's sign. • 100% is associated or followed with malignancy especially in Old male. : bronchogenic carcinoma & ovarian malignancy In females : breast and ovarian malignancy
- 39. Investigations : 1. CPK: increased 10 times, in acute state. 2. ESR: increased . 3. EMG: mixed myopathic and neurogenic (fibrillations at rest) patterns. 4. Muscle biopsy "Inflammatory changes" see i_mmunopathogenesis. 5. look for associated auto immune disease: RF, anti DNA. 6. Investigations for hidden malignancy. 7. MRI may help identify patients with autoimmune myopathy.
- 40. Treatment : 1) Steroids: large doses: • Prednisone 60 mg/day for 2-3 weeks. • Gradually reduce the dose to 40 mg/day. • Gradually decrease the dose guided by CPK levels and clinical response. • Maintenance therapy for several years. • Pulse dose (high dose) steroids may be required for a short period. 2) Immunosuppressive therapy: • Cyclophosphamide or Azathioprine, Methotrexate or Chlorambucil. Usually combined with steroids from the start. • Cyclosporine A may be beneficial in resistant cases. 3) Intravenous immunoglobulin: is very effective but costy. 4) Plasmapheresis: is useful in acute cases.
Editor's Notes
- #31: 2.4 to 5.5 per 100,000 population Inherited Autosomal Dominant Treatment is symptomatic
- #32: High perioperative morbidity and mortality are caused pricipally by cardiopulmonary complications
- #33: Characteristic triad of mental retardation, frontal baldness, cataract fomration. Also see expressionless facies secondary to facial weakness Wasting and weakness of sternocleidomastoid muscles ptosis