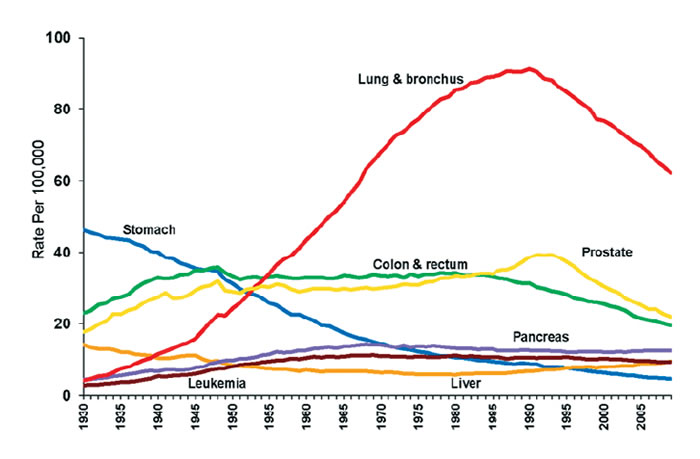
They're not very similar. The nuclear tests graph starts at 0 at 1950 (when the cigarettes-smoked graph is three-quarters of the way to its peak). Lung cancer incidence has been rising steadily and pretty much linearly since the 30's, until the 80's.
If nuclear tests are the main reason for lung cancer, then why did lung cancer incidence start rising before nuclear weapons were invented?
If nuclear tests are the main reason for lung cancer, and their effect is due to background radiation, why weren't all cancers increasing steadily rather than simply lung cancer?
>"If nuclear tests are the main reason for lung cancer, then why did lung cancer incidence start rising before nuclear weapons were invented?"
It became easier to diagnose, or perhaps more trendy? It is actually really hard to distinguish between lung cancer and tuberculosis.[1] At ref 2 you can see tuberculosis rates dropping from 200/100k in 1900 to near 0 in 1980. In the meantime lung cancer rose from near 0 to ~100/100k deaths.[3]
Also, as I mentioned, there was a fad to expose yourself to radioactive stuff starting about 1900 that only died out in the 1960s.[4]
So, could be lots of things in combination.
>"If nuclear tests are the main reason for lung cancer, and their effect is due to background radiation, why weren't all cancers increasing steadily rather than simply lung cancer?"
My understanding is they were.[5] The lungs may especially vulnerable to radioactive dust though, if they had already "accounted for", as the lung cancers due to smoking, then this could have been missed.
The usual strategy is to control for smoking. If nuclear test rate correlates with lung cancer rate, but does not correlate with non-smoker lung cancer rate, nuclear test is not causing lung cancer.
Epidemiology is a field of study about how to do this right. One of the great achievement of humanity in the 20th century was advance of epidemiology.
>"the lung cancer mortality rate has risen substantially between 1914 and 1968 among persons who never smoked cigarettes. For white males the relative increase for ages 35--84 years has been about 15-fold; the relative increase for ages 65--84 years has been about 30-fold."https://www.ncbi.nlm.nih.gov/pubmed/285289
Yup, epidemiology of non-smoker lung cancer is an active area of research. (Epidemiology of smoker lung cancer is not; it's very well established.) I haven't seen this old article, but it sounds perfectly right; the quoted result is probably due to diagnostic criteria.
Lung cancer in never smokers (2009) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3170525/ shows the field in confusion. Radon, indoor air pollution, second-hand smoking are named as possible sources, but it's still not satisfactory.
That's interesting -- doesn't seem to have a graph, but states a significant increase between 1914 and 1967 in nonsmokers. There doesn't appear to be any control for secondhand smoke, however, which could also be a significant factor over that time period.
Sure, another thing to consider is fallout incorporated into tobacco and then smoked...
But do you see why I didn't care if a correlation existed? There are a bunch of ways to explain such a correlation. That line of reasoning was based on the affirming the consequent fallacy[1]:
If
H: Nuclear tests are a significant factor in lung cancer rate
Then
O: We should still see a correlation between lung cancer incidence and nuclear test frequency [in non-smokers]
We can't conclude "O is true, therefore H" (since there are a million potential reasons for O besides H), so we don't learn anything from it. Now if O had been some very specific prediction unlikely to arise from other hypotheses, I would care.
In terms of Bayes' Rule, I only care if p( O|H[0] ) dominates all the other possibilities (H[1:n]) in the denominator. The mere existence of a positive correlation isn't specific enough for me to care:
Yes, epidemiology is not deductive, and in the end it depends on whether observation is "specific enough" for you st unlikely to arise from other hypotheses, which in turn depends on your prior, which is informed by laboratory results in addition to field results. Epidemiology is a truly fascinating subject.
Affirming the consequent is a deductive fallacy. It is not a fallacy in probabilistic reasoning, because the consequent is an evidence of the antecedent.
Re: laboratory results, it is noteworthy smoking and non-smoking lung cancer have different molecular signature. Lung cancer probably should be considered two separate diseases, and this probably overstates smoking connection because some lung cancer by smokers is of non-smoking kind and not caused by smoking. This can be better understood by including such signatures in epidemiological study.
>"Affirming the consequent is a deductive fallacy. It is not a fallacy in probabilistic reasoning"
Nevertheless, people commit that fallacy all the time in epidemiology. They say stuff like "if smoking caused cancer, then people who smoked would get cancer more often". Then if there is a (statistically significant) positive correlation between cancer and smoking, they conclude smoking causes cancer.
That is quite obviously affirming the consequent. I explain the (completely different and correct) probabilistic way to think about this situation using Bayes' rule in my post.
It has nothing to do with arbitrary cut-offs for telling us whether a correlation exists or not. Instead it requires comparing the relative performance of the various explanations (at least the top few candidates since extremely unlikely ones can be dropped from the sum in the denominator).
I don't think anyone serious about epidemiology says stuffs like that. On the other hand, it is true many people interpret what epidemiology says as such.
Saying smoking is a risk factor of cancer is very different from smoking causes cancer. As you said, you must consider alternative explanations. On the other hand, people can disagree about what alternative explanations are "extremely unlikely" and "can be dropped", that's what I meant by prior. For example, nuclear test causes cancer, is probably extremely unlikely.
Smoking being a risk factor of cancer is an evidence of smoking causing cancer. Being evidence of causal relation is completely different from being sufficient to prove causal relation.
Definitely, but if O had been false we might have learned something. More interestingly though:
> another thing to consider is fallout incorporated into tobacco and then smoked
That's an interesting thought, I'd never considered that.
My expectation for beta and gamma emitters is that they would be unlikely to cause cancer specifically in the lungs, because lungs aren't very dense and would have a pretty low interaction cross section for such penetrating radiation. For comparison, I-131 -- a beta emitter common in fallout -- is a significant risk for thyroid cancer only because iodine is biologically concentrated in the thyroid.
However, if there were significant fallout of alpha emitters, which were deposited in tobacco, this could conceivably deliver a significant localized dose to the lungs. Alpha emitters are more or less only dangerous internally, but smoke particulates that become lodged in the lungs could do the job. There appears to be a fair amount of literature on this -- Naturally occurring Po-210 is apparently still considered a danger today [1], and has been known to the cigarette companies since the 60s [2]. Some apparently comes from decay of natural U (via a few intermediaries) in phosphate fertilizer.
A figure in one paper I was able to find [3] suggests up to 100 pCi/kg Pu-239 and Pu-240 (both alpha) in leaves and grass in Finland circa 1963, declining to less than 5 pCi by 1967. The modern Po-210 alpha activity in tobacco appears to be much higher than either of these values (perhaps several hundred pCi/kg in dry tobacco, if not more), but I couldn't find good data on variation over time. For Pb-210 (beta) there is more data, but seems to be a lot of scatter and not so much of a clear trend through time [4].
>"The usual strategy is to control for smoking. If nuclear test rate correlates with lung cancer rate, but does not correlate with non-smoker lung cancer rate, nuclear test is not causing lung cancer."
I'm not really concerned with whether there is, or is not, a correlation, I already know there is a correlation.
I am concerned about: How much of the increase in lung cancer incidence we see in the data could be accounted for via exposure to radiation from nuclear tests? I doubt it is zero, but it could be relatively negligible I suppose.
This is missing their point: you can distinguish the two potential causes by comparing lung cancer incidence rate through time for smokers versus non-smokers.
If nuclear tests are a significant factor in lung cancer rate, we should still see a correlation between lung cancer incidence and nuclear test frequency when looking at people with no exposure to cigarette smoke. If the correlation in the general population just a coincidence, we should not.
{kind=link}
{kind=link}
Looked eerily similar to this one: https://i.ibb.co/cLbTRfM/nuctest.png
Source for nuclear test data: https://www.armscontrol.org/factsheets/nucleartesttally
And before there were nuclear tests, there was a big fad to expose yourself to radiation early in the 1900s: https://www.popsci.com/scitech/article/2004-08/healthy-glow-...
Is the argument that the nuclear tests, etc had zero effect on lung cancer rates? If not, what was it?